Burkholderia Cepacia
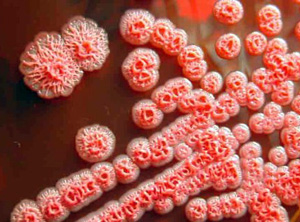
Morphology and culture
The name of Burkholderia cepacia (formerly Pseudomonas cepacia) is derived from the American microbiologist Walter Burkholder, who first isolated in 1950 from the seed rotting onion bulbs. Today, under the name of Burkholderia cepacia complex are at least ten closely related species combined (Genomovare) that are simplistically referred to as Burkholderia cepacia. It is about 1 x 2.5 microns great aerobic gram-negative bacilli with polar flagella. The Burkholderiaarten are like the pseudomonads not able to utilize carbohydrate and therefore be associated with the so-called "non-fermenters". The detection of the pathogen in routine microbiological laboratory is due to the genotypic and phenotypic diversity difficult (see below).
Pathogenesis and clinical pictures
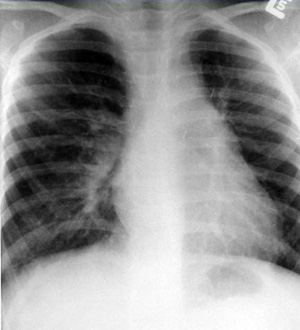
Burkholderia cepacia is a primarily plant pathogenic germ, which occurs in humid conditions in the soil. The natural habitat is water and Knoll area of vegetables (z. B. onions) and other plants. Once in the 70s initially only reports on the detection of Burkholderia cepacia in cystic fibrosis patients (synonym: Cystic fibrosis) had appeared in 1984 in Toronto (Canada) for the first time a endemieartiges presence of the pathogen in CF patients with T z. known. severe infections. Burkholderia cepacia is now considered one of the most important pathogen in CF patients. In addition, he has been described as a cause of pneumonia in patients with chronic granulomatous disease and as a nosocomial pathogen in immunocompetent patients.
The transmission is airborne as a rule. Here, with Burkholderia cepacia populated patients pose the greatest risk for transmission. In the private sector, contamination via the ingestion of water or plant parts are carried out. The main source of infection in hospitals represent contaminated disinfectant. The settlement takes place in the respiratory tract where the pathogens with the help of pili and other factors adheres to epithelial cells, in which he can then penetrate and multiply there. The exact mechanisms have not yet been clarified.
The disease can be very different. In most patients, the lung function does not deteriorate while in 20% of cases, acute necrotizing pneumonia with sepsis running occurs (so-called Burkholderia cepacia syndrome). In this case, the course of the infection to one of the virulence of the pathogen and the other seems to be determined by the individual factors of the affected CF patients.
Because in comparison to Pseudomonas aeruginosa significantly higher infectivity populated with Burkholderia cepacia CF patients must not come into contact with other CF patients.
Burkholderia Cepacia therapy
The therapy usually includes multiple antibiotics. The highest sensitivity rates were reported for ceftazidime (FORTUM) and piperacillin / tazobactam (Tazobac); the carbapenems, tetracyclines, fluoroquinolones and chloramphenicol are partially effective in vitro. However, the in vitro activity has only a low predictive value for therapeutic use in CF patients because the pathogen elimination from the sputum usually do not succeed in vitro effective antibiotics also. The cause for this observation is the ability of pathogens to form biofilms into consideration. The most important therapeutic measure thus constitutes the consequent bronchial.
| Name | Dosage | |
| Ceftriaxone | 1 - 2 g | once a day not more than 10 days. The introduction of the drug is recommended to continue for another 2-3 days after normalization of body temperature and symptoms disappear. |
| Grepafloxacin | 400 - 600 mgs | once a day for 7 - 10 days |
|
Burkholderia Cepacia diagnosis and prevalence of resistance
The detection of the pathogen is done by growing from Respirationstraktmaterialien. However, the identification is not easy. When using the usual commercial test procedures or selective media Burkholderia cepacia were often identified or overlooked wrong. Although the use of specific phenotypic tests helps to better define, in particular Burkholderia gladioli to, Stenotrophomonas maltophilia or Ralstonia spp .; but for an unambiguous assignment of bacteria to the genomovars of Burkholderia cepacia complex, the application of molecular biological methods is required.
Burkholderia cepacia is characterized by a resistance to many antibiotics. Naturally, there is a resistance to aminoglycosides and polymyxins. In addition, there is usually a resistance to many beta-lactam agents that is based on the production of chromosomally-encoded beta-lactamases or altered penicillin binding proteins.
|

